SIGNATURE CLINICAL CASE
When Shin Pain Is Not a Shin Problem
A fascia-based Cross Pattern case showing how persistent anterior shin pain during running may reflect a deeper failure in load transmission.
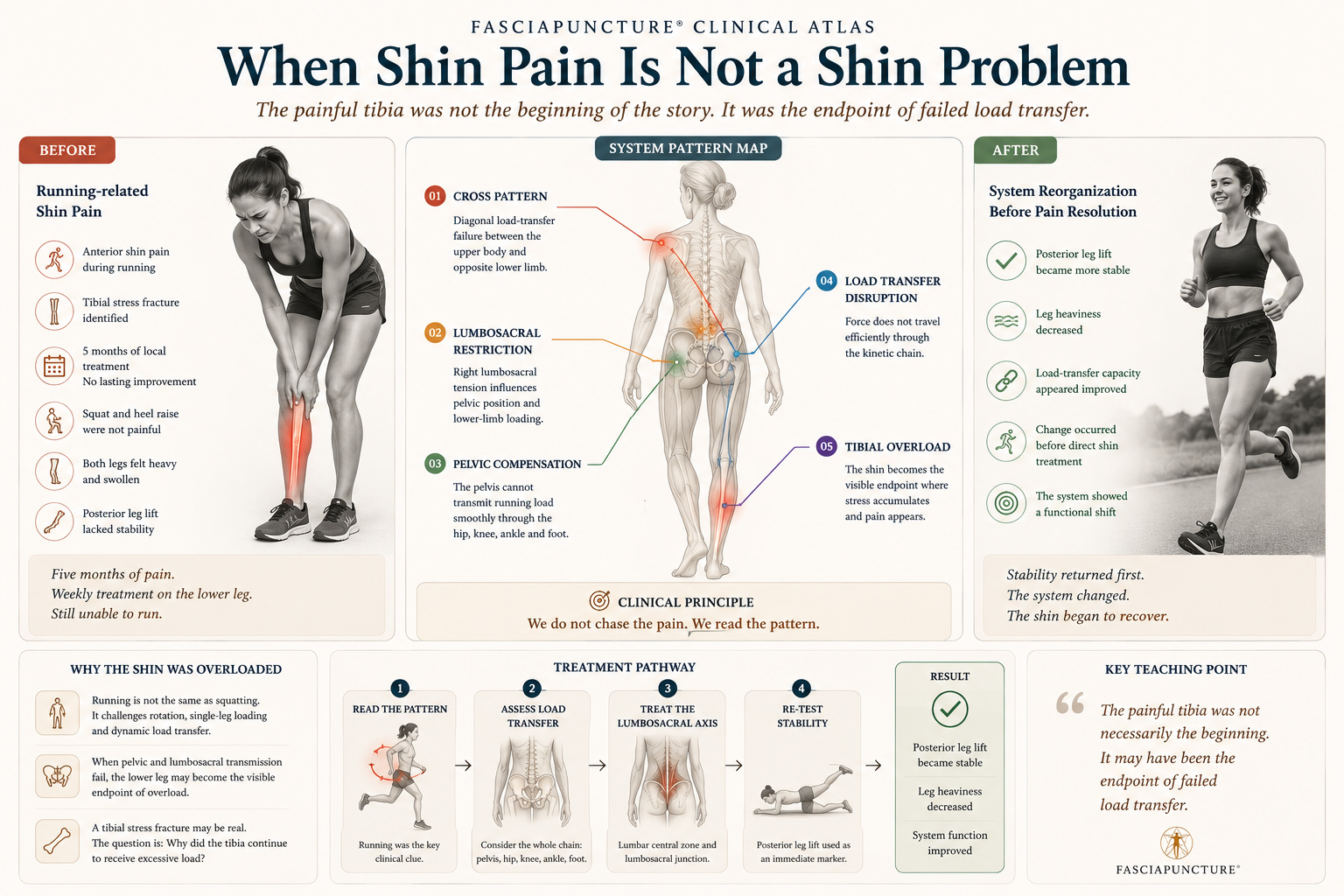
The shin carried the load. The pattern carried the problem.
CLINICAL OPENING
The painful tibia was not necessarily the origin
A 29-year-old woman presented with persistent anterior shin pain during running. A tibial stress fracture had been identified, yet five months of local treatment did not restore her ability to run.
She had received weekly physiotherapy and massage focused on the lower leg, but no lasting improvement occurred. Squat and heel raise were not painful, while running continued to provoke symptoms.
INITIAL SYSTEM STATE
What the body showed before treatment
Main Presentation
- Female, 29 years old
- Anterior shin pain during running
- Duration: five months
- Tibial stress fracture identified
- No lasting improvement after local care
Functional Clues
- Squat was not painful
- Heel raise was not painful
- Running remained symptomatic
- Both legs felt heavy and swollen
- Posterior leg lift showed reduced stability
PATTERN ATLAS
The shin was the endpoint of a failed load-transfer pattern
Cross Pattern
The symptoms suggested a diagonal load-transfer failure rather than an isolated lower-leg dysfunction.
Lumbosacral Restriction
Right lumbosacral tension appeared as a key restriction zone influencing lower-limb loading.
Pelvic Compensation
The pelvis appeared unable to transmit running load smoothly through the hip, knee, ankle, and foot.
Lower Limb Overload
The painful tibia may have become the place where unresolved global load finally appeared.
BEFORE & AFTER CLINICAL ATLAS
Stability returned before pain disappeared
Before
- Running-related anterior shin pain
- Five months of persistent symptoms
- Local treatment focused on the lower leg
- Both legs felt heavy and swollen
- Posterior leg lift lacked stability
After
- Posterior leg lift became more stable
- Leg heaviness decreased
- Load-transfer capacity appeared improved
- Change occurred before direct shin treatment
- The system showed a functional shift
ENTRY STRATEGY
The treatment followed the pattern, not the pain
Read the Running Pattern
Running was used as the key clinical clue because it challenged rotation, single-leg loading, and whole-chain coordination.
Assess Load Transfer
The pelvis, lumbosacral region, hip, knee, ankle, and foot were considered as one transmission system.
Treat the Lumbosacral Axis
The lumbar central zone and lumbosacral junction were prioritized instead of chasing the painful shin.
Re-Test Stability
Posterior leg lift was re-tested as an immediate marker of system-level load-transfer change.
CLINICAL TURNING POINT
The shin changed when the load-transfer system changed
The treatment did not focus on the painful shin. Instead, the intervention followed the Cross Pattern and targeted the areas where the system appeared blocked: the lumbar central zone, the lumbosacral junction, and the diagonal load-transfer axis.
After treatment, posterior leg lift became noticeably more stable. The patient also reported a reduction in the sensation of heaviness in the legs.
WHAT BECAME VISIBLE
Observable signs of functional change
Stability
Posterior leg lift became noticeably more stable.
Leg Heaviness
The patient reported less heaviness in both legs.
Load Transfer
The system appeared better able to transmit force through the lower limb.
Pain Logic
The shin was no longer interpreted as an isolated local structure.
Clinical Direction
The case shifted from local treatment to pattern-based reasoning.
CLINICAL REFLECTION
The fracture may not be the beginning of the story
This case illustrates a core principle in Fasciapuncture® clinical reasoning: a local diagnosis can coexist with a systemic dysfunction.
Local treatment may be necessary. But when it fails repeatedly, the clinician must ask what pattern keeps sending stress to the same region.
KEY LEARNING POINTS
What this case teaches
Running is not the same as squatting
Squatting and heel raising are symmetrical. Running challenges rotation, single-leg loading, and dynamic load transfer.
Local diagnosis is not the whole map
A tibial stress fracture may be real, but the clinical question remains: why did the tibia continue to receive excessive load?
The pelvis may decide the shin
When pelvic and lumbosacral transmission fail, the lower leg may become the visible endpoint of overload.
Functional testing guides treatment
Posterior leg lift helped reveal whether the system’s load-transfer capacity had shifted.
CONNECTED CLINICAL MAP
Patterns connected to this case
Compensation Loop
Repeated load redistribution that keeps sending stress to the same region.
Pelvic Lock
Restricted pelvic transmission affecting gait, load, and lower-limb mechanics.
Posterior Compression
Lumbosacral restriction, posterior-chain pressure, and limited extension capacity.
Lower Limb Load Transfer
How the hip, knee, ankle, foot, and tibia receive force during running.
RELATED CONDITIONS
Conditions connected to this case
RELATED CASES
Other cases where load transfer became visible
When the Spine Begins to Rise Again
Posterior overload, abdominal compensation, and visible spinal reorganization.
The Foot Was Not the Problem
A case where foot pain revealed a larger lower-limb and pelvic transmission pattern.
When the Abdomen Finally Let Go
Abdominal holding, breathing restriction, and pelvic protection.
CONTINUE LEARNING
From local shin pain to pattern recognition
Module 2 — Clinical Perception & Diagnosis
Learn functional testing, movement reading, and pattern recognition.
Module 10 — Lower Limb Disorders
Explore thigh, knee, shin, calf, ankle, and foot load-transfer patterns.
Module 1 — Foundations of Fasciapuncture®
Understand why pain may be the endpoint of a deeper adaptation.
