SIGNATURE CLINICAL CASE
After Wrist Surgery, the Problem Was No Longer the Wrist
A fascia-oriented clinical case showing how chronic post-surgical arm pain, breathing restriction, and anterior collapse may become part of a global protective pattern.
CLINICAL OPENING
The symptom was local. The adaptation was global.
A 77-year-old woman presented with persistent pain following left wrist surgery performed two years earlier. Over time, the symptoms progressively expanded beyond the wrist and began affecting the entire upper body.
She described constant tension extending from the wrist into the arm, shoulder, and neck, associated with breathing difficulty, sleep disturbance, physical fatigue, tinnitus, and constipation.
INITIAL SYSTEM STATE
What was visible before treatment
Main symptoms
- Persistent left wrist and arm pain
- Neck tension and restricted mobility
- Shortness of breath
- Chest tightness
- Insomnia
- Tinnitus
- Constipation
Aggravating factors
- Prolonged tension after surgery
- Difficulty relaxing the upper body
- Protective breathing pattern
- Persistent anterior loading posture
- Fatigue and poor recovery during sleep
PATTERN ATLAS
The wrist was part of a larger protective organization
Upper Exit Block
Neck, thoracic outlet, shoulder, and arm tension suggested that the upper body had become a restricted exit zone.
Anterior Chain Lock
Forward head posture, collapsed thorax, and anterior arm positioning showed a global anterior holding pattern.
Diaphragm Restriction
Breathing difficulty and chest tightness indicated that respiratory mechanics were involved in the pain pattern.
Autonomic Dysregulation
Insomnia, tinnitus, constipation, and fatigue suggested that the system was no longer returning easily to regulation.
BEFORE & AFTER CLINICAL ATLAS
When the arm relaxed, the whole posture changed

Before
- Forward head posture
- Collapsed upper thorax
- Anterior arm positioning
- Reduced respiratory expansion
- Protective upper-body flexion
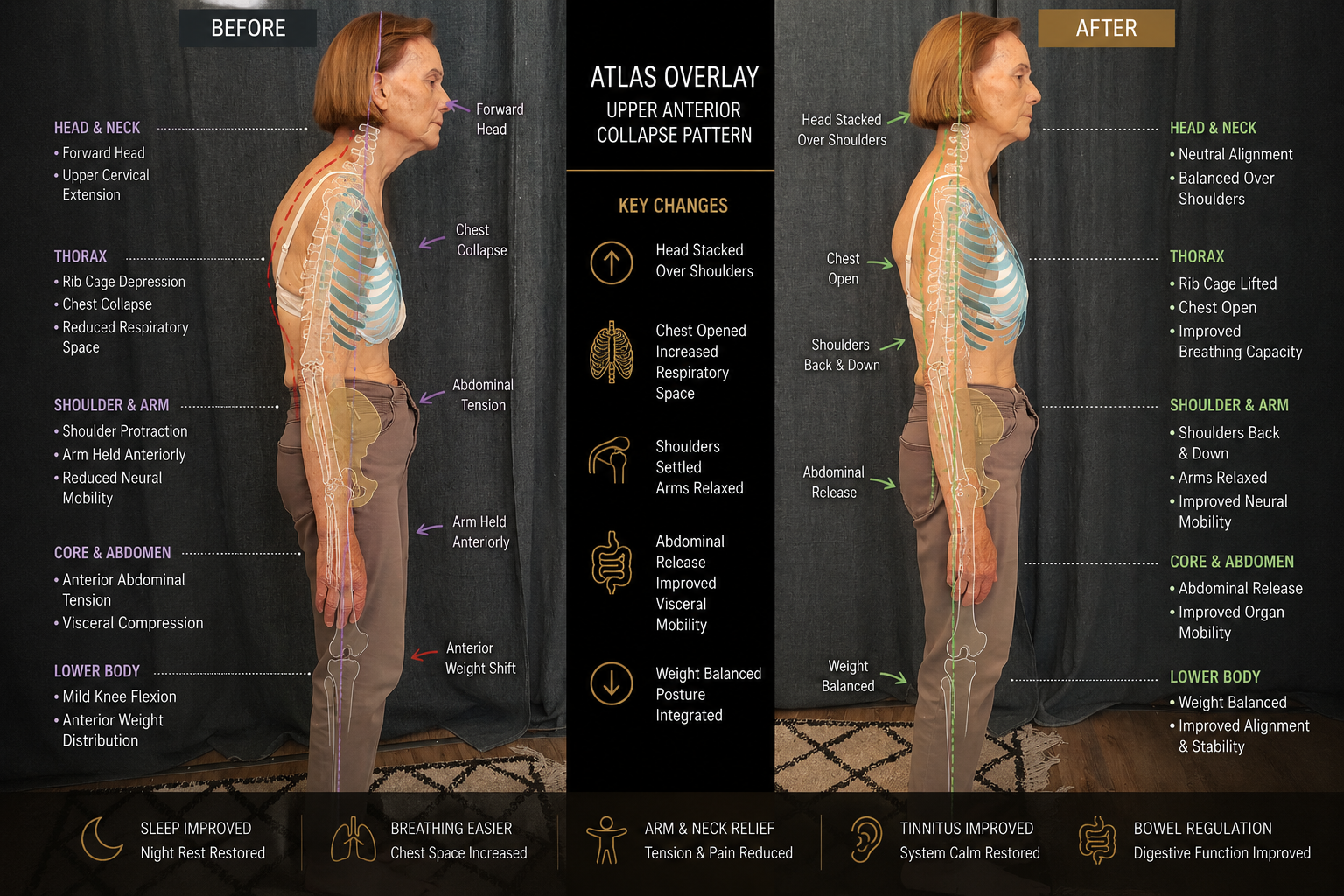
After
- Chest appeared more open
- Breathing became deeper
- Arm tension reduced
- Posture reorganized spontaneously
- Upper body felt lighter
ENTRY STRATEGY
Treating the system before forcing the symptom
Upper Entry
Anterior cervical region, thoracic outlet, and respiratory decompression were used to reduce the upper exit restriction.
Central Axis
Mid-abdominal regulation and diaphragmatic tension reduction helped unload the anterior fascial chain.
Arm Without Force
The painful arm was not forced directly. It was allowed to relax as breathing, thoracic pressure, and global tension changed.
CLINICAL TURNING POINT
When breathing returned, the arm began to let go
Instead of treating the wrist as the primary problem, the intervention focused on restoring respiratory and fascial regulation through key entry zones.
As breathing became easier and the chest opened, the arm tension significantly reduced. The change was visible not only in pain expression, but in posture, respiratory space, and upper-body lightness.
WHAT BECAME VISIBLE
Observable signs of regulation
Breathing
Respiration became deeper and easier.
Arm Tension
The upper limb began to release without direct forcing.
Posture
The anterior collapse visibly reduced.
Chest
The thoracic region appeared more open.
System State
The patient reported lightness in the upper body.
CLINICAL REFLECTION
Pain is not always where the dysfunction begins
Chronic post-surgical pain may evolve into a global adaptive pattern involving breathing, posture, autonomic regulation, and fascial tension distribution.
In this case, restoring respiratory and fascial regulation allowed the arm to relax naturally — without directly forcing the painful area.
KEY LEARNING POINTS
What this case teaches
Local pain can become systemic
A surgical history may begin locally but later organize breathing, posture, and autonomic regulation.
The arm may be held by the trunk
When thoracic pressure and diaphragmatic restriction shift, upper-limb tension may reduce naturally.
Breathing is a clinical marker
Breath change is often one of the earliest signs that the protective pattern is softening.
Do not chase the symptom
The best entry point may be where the system can regulate, not where the pain is loudest.
CONNECTED CLINICAL MAP
Patterns connected to this case
Upper Exit Block
Neck, thoracic outlet, shoulder, arm, and skull-base pressure organization.
Anterior Chain Lock
Forward collapse, anterior fascial shortening, and restricted extension.
Diaphragm Restriction
Breathing limitation, chest pressure, and regulatory load.
Autonomic Dysregulation
Sleep, tinnitus, digestion, and system recovery difficulty.
RELATED CONDITIONS
Conditions connected to this case
RELATED CASES
Other cases where the system became visible
When Breathing Becomes Quiet
A clinical moment where breathing descends and the system softens.
When the Abdomen Finally Let Go
A case of abdominal holding, breathing restriction, and pelvic protection.
When the Spine Begins to Rise Again
Posterior overload, abdominal compensation, and visible spinal reorganization.
CONTINUE LEARNING
From local pain to global pattern reading
Module 1 — Foundations of Fasciapuncture®
Learn how symptoms become readable through fascia-oriented clinical reasoning.
Module 2 — Clinical Perception & Diagnosis
Learn to read posture, breathing, pressure, and systemic regulation.
Cranio-Cervical and Shoulder Syndromes
Explore upper-body patterns, neck tension, shoulder load, and arm symptoms.
