1 Patient Profile
-
Age: 42
-
Sex: Female
-
Main Complaint: Jaw tension with audible clicking, cervical and medial scapular pain
-
Duration: Several months
-
Trigger / Onset: Progressive tension associated with stress and poor sleep
-
Previous Treatments: None with lasting improvement
The patient reported persistent jaw tightness and frequent stretching movements of the mouth to relieve tension. Clicking sounds occurred during jaw opening. At the same time, she experienced pain along the right cervical region and the medial border of the scapula. Sleep had become lighter and more fragmented, accompanied by feelings of anxiety and internal pressure.
Summary
The patient sought Fasciapuncture® after persistent symptoms affecting daily comfort, sleep quality, and emotional balance.
2 Clinical Observation
Palpation and observation revealed several zones of fascial tension:
-
Increased tension along the cervical–scapular fascial corridor, particularly on the right side
-
Local sensitivity near the levator scapulae and upper trapezius fascial insertion
-
Tension in the suprahyoid–submandibular fascial area, associated with jaw tightness
-
Mild postural forward-head pattern with increased cervical loading
No structural joint pathology of the temporomandibular joint was suspected.
The pattern suggested a functional fascial tension network rather than isolated joint dysfunction.
3 Fascia-Based Interpretation
From a fascial perspective, the symptoms formed a coherent pattern.
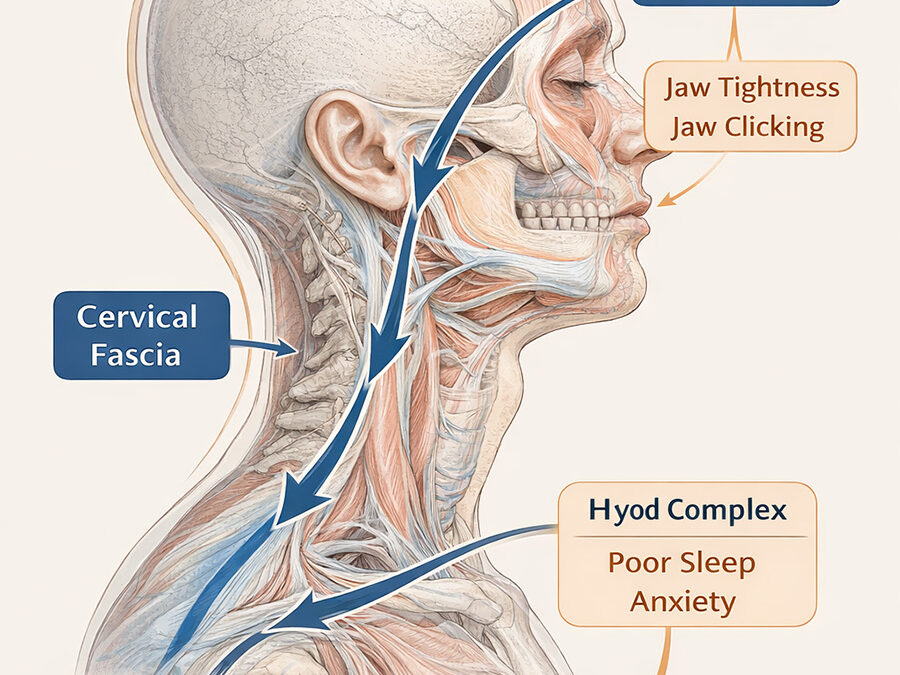
The cervico-scapular fascia plays a key role in transmitting tension between the shoulder girdle, cervical spine, and craniofacial structures. When tension accumulates in this corridor, it may influence the hyoid complex and mandibular fascial system, altering the balance of the temporomandibular region.
This type of tension pattern can also interact with the autonomic nervous system, contributing to:
-
jaw tightening
-
sleep disturbance
-
heightened internal tension or anxiety
In this case, the jaw clicking and tightness were interpreted not as a primary jaw disorder but as a distal manifestation of cervico-fascial tension.
Summary
The jaw symptoms appeared locally, but the tension pattern originated primarily within the cervico-scapular fascial system.
4 Treatment Strategy
The treatment approach followed a fascia-oriented regulation strategy rather than focusing directly on the jaw.
The intervention aimed to:
-
reduce tension within the cervical fascial layers
-
restore mobility in the scapular fascial corridor
-
release associated fascial tension around the submandibular and upper thoracic regions
-
support global regulation of the autonomic system
The goal was not aggressive mechanical correction but precise fascial decompression to allow the system to reorganize naturally.
5 Clinical Response
The patient showed rapid functional changes during and shortly after the session.
Observed responses included:
-
disappearance of the jaw clicking sound
-
reduction of cervical and medial scapular pain
-
visible relaxation of facial tension
-
subjective feeling of reduced internal pressure
The patient reported feeling lighter and calmer, and her facial expression visibly softened during the session.
6 Physiological Interpretation
Fascial tissues form a continuous network linking the cervical region, hyoid structures, and craniofacial system. When excessive tension accumulates in this network, mechanical stress and altered sensory input may propagate to distant structures such as the temporomandibular region.
By restoring mobility within the primary tension zones, mechanical load and neural sensitivity may rapidly decrease in distal areas.
Summary
Treat the origin → the distal endpoint often changes first.
7 Clinical Insight
Clinical Reflection
Jaw clicking and mandibular tension are frequently treated as isolated temporomandibular joint problems. However, in many patients the underlying driver lies in cervical and scapular fascial tension patterns.
Understanding these relationships allows clinicians to intervene at the primary regulatory zones rather than chasing secondary symptoms.
Distal symptoms often reflect proximal fascial tension rather than local pathology.

