SIGNATURE CLINICAL CASE
When the Pain Memory Disappeared
A herpes zoster case where acute neuropathic pain, skin lesions, and the emotional memory of suffering gradually faded as the neuro-fascial system recovered regulation.
CLINICAL OPENING
The pain was acute, but the system was overwhelmed.
A 75-year-old female patient came during an acute herpes zoster episode. The pain was severe, piercing, and deeply exhausting. She described it as if “one thousand needles were piercing the body at the same time.”
The herpes zoster eruption was located around the lumbosacral region, with intense neuropathic pain extending toward the abdomen.
The goal was not to treat the skin lesion directly, but to calm the neuro-fascial environment surrounding the irritated nerve pathway.
INITIAL SYSTEM STATE
The Nervous System Was in a State of Alarm
Patient Profile
- 75-year-old female patient
- Recently developed acute herpes zoster
- Severe pain around the lumbosacral dermatome
- Emotional stress before the outbreak
Pain Presentation
- Sharp neuropathic pain
- Marked skin hypersensitivity
- Pain extending toward the abdomen
- Difficulty sitting still because of pain intensity
Clinical Observation
- Protective muscle contraction
- Fascial tension around the affected segment
- Heightened nervous system reactivity
- Guarding around the lumbosacral region
Systemic State
- Anxiety and sleep disturbance
- Overactive pain perception
- Reduced ability to relax
- Strong emotional imprint of suffering
PATTERN ATLAS
Patterns Revealed in This Case
Neuro-Fascial Irritation
The irritated nerve pathway appeared amplified by surrounding fascial hypersensitivity.
02Autonomic Dysregulation
Pain, stress, and sleep disturbance reflected a nervous system unable to return to safety.
03Posterior Compression
The lumbosacral region carried protective tension around the affected dermatome.
04Inflammatory Overload
The acute inflammatory state increased sensitivity across the local neuro-fascial field.
ZOSTER REGULATION ATLAS
The Skin Was Only the Surface of the Story
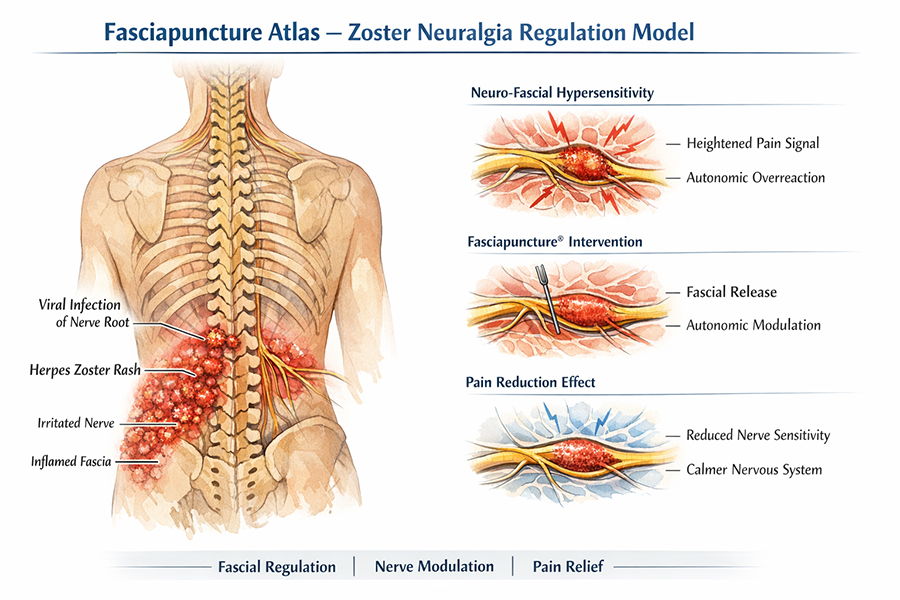
Herpes zoster pain was interpreted through the interaction between viral irritation, nerve hypersensitivity, fascial tension, and autonomic overactivation.
ENTRY STRATEGY
Treatment Did Not Begin at the Skin Lesion
THE CLINICAL TURNING POINT
The First Change Was Not the Skin
During the treatment, the patient reported a rapid decrease in pain intensity. The pain level dropped by approximately 50% during the session.
For the first time since the outbreak, she felt she could breathe more easily and relax her body. The immediate reduction in pain gave her a renewed sense of hope.
WHAT BECAME VISIBLE
The System Calmed Before the Skin Recovered
FOLLOW-UP VIDEO
One Year Later, the Pain Was No Longer Part of Her Story
The patient later became a regular long-term client together with her husband. More than one year after the acute herpes zoster episode, the pain had not returned.
Follow-up video: the patient speaks about her recovery and how the painful memory of the episode has disappeared.
LONG-TERM EVOLUTION
The Scar Faded. The Pain Memory Faded Too.
Over time, the acute herpes zoster pain resolved completely. The skin lesions healed, and even the visible scars gradually disappeared.
More importantly, the patient no longer carried the painful memory of the episode. What had once been an overwhelming experience became something distant, no longer emotionally present in the body.
The treatment did not only reduce pain. Over time, the body no longer carried the memory of pain.
CLINICAL REFLECTION
Pain Can Leave a Trace Beyond the Skin
Herpes zoster is often understood through the viral eruption and the visible skin lesions. Yet in this case, the suffering was not limited to the dermatological presentation.
The body had entered a state of neuro-fascial hypersensitivity: nerve irritation, fascial guarding, autonomic overactivation, and emotional fear were all present at the same time.
Fasciapuncture® did not replace medical care for the viral condition. It offered a complementary clinical perspective by addressing the regulatory environment around the irritated nerve pathway.
When the nervous system calms, pain may stop being the center of the body’s story.
CONNECTED CLINICAL MAP
Explore Related Conditions & Patterns
RELATED CASES
Other Cases in the Same Clinical Map
CONTINUE LEARNING
From Pain Relief to Neuro-Fascial Regulation
Foundations of Fasciapuncture®
Understanding regulation before intervention.
Module 2Clinical Assessment
Reading global patterns instead of isolated symptoms.
Module 8Lumbar & Sacral Fascia
Understanding lumbosacral regulation and posterior chain responses.
TrainingClinical Reasoning Pathway
Learn how cases become maps for clinical decision-making.