FASCIAPUNCTURE® SIGNATURE CLINICAL CASE
When the Low Back Was the Last Place to Complain
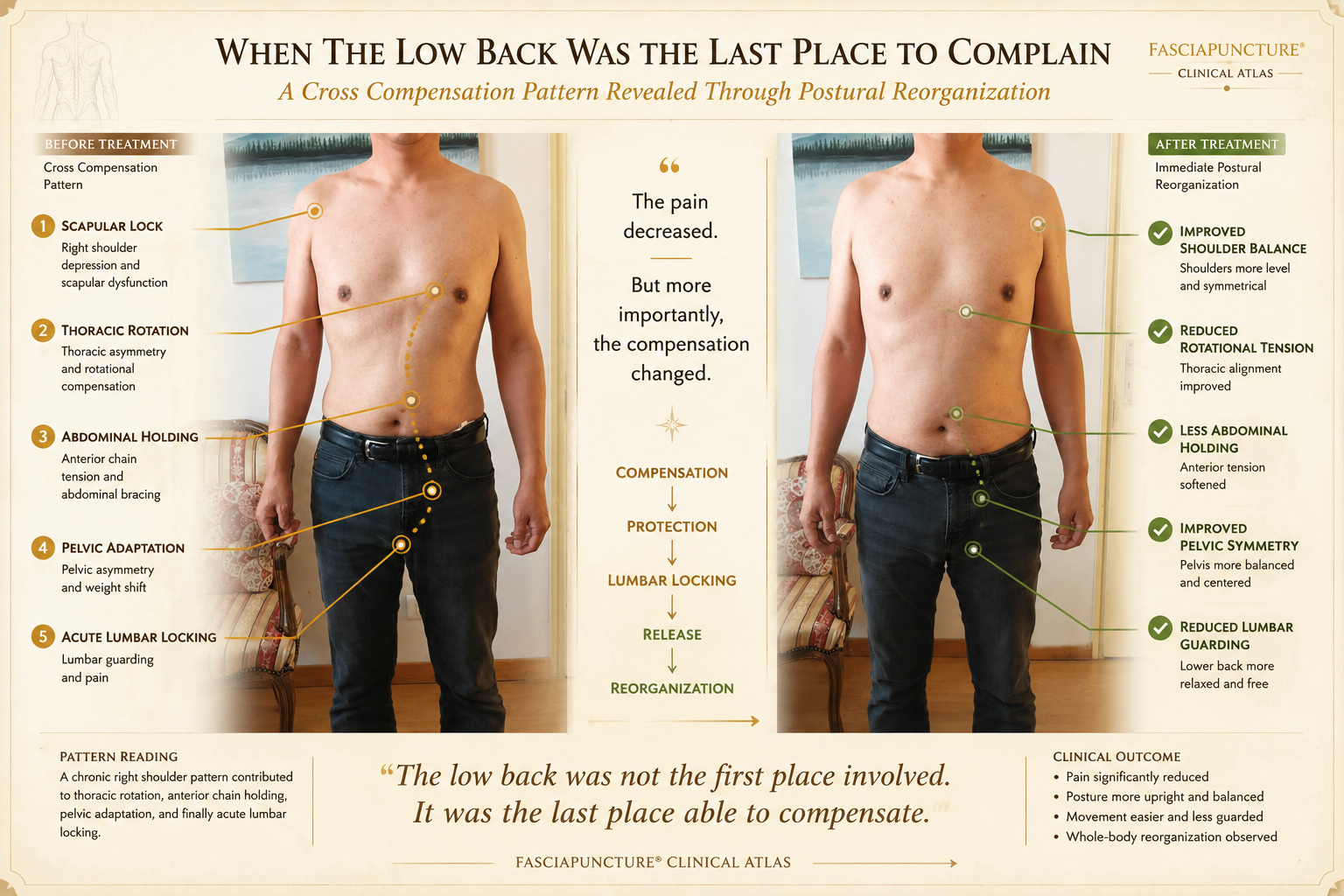
A clinical case of acute lumbar locking associated with chronic right shoulder compensation, anterior chain collapse, and cross-pattern release.
CLINICAL OPENING
The pain was acute, but the pattern was not new.
The patient operated a small family grocery store with his wife. His daily work was physically demanding: lifting boxes, carrying supplies, organizing shelves, standing for long hours, and managing the checkout counter.
When the low back suddenly locked, continuing to work became difficult. Standing upright was painful, walking felt guarded, and lumbar extension increased discomfort.
At first glance, the problem seemed local. But the patient also had a history of right shoulder pain. This detail changed the clinical reading.
The lumbar region appeared to be the final place where a longer compensatory pattern had reached its limit.
BEFORE & AFTER CLINICAL ATLAS
What changed first?
Anterior chain collapse decreased. Abdominal holding softened. Vertical alignment improved.

Posterior View
Shoulder asymmetry reduced. Trunk balance improved. Weight distribution became more centered.

Side View
Visible changes in posture, balance, and protection patterns appeared immediately after treatment.
Front View
Lumbar guarding reduced. Pelvic adaptation became less visible. Cross-compensation tension decreased.
INITIAL SYSTEM STATE
A body protecting itself under daily load
Daily Load
The patient worked long days in a small family grocery store. His routine involved lifting boxes, moving supplies, stocking shelves, standing at the checkout counter, and repeating these tasks throughout the day.
Visible Postural Signs
Right shoulder depression, trunk asymmetry, anterior collapse, abdominal holding, pelvic imbalance, and lumbar guarding were visible.
Clinical Context
The history of right shoulder pain suggested that the lumbar episode was not isolated, but connected to a longer upper-body compensation.
System Reading
The body appeared locked in a cross-compensation strategy, using the shoulder, thorax, abdomen, pelvis, and lumbar region as one adaptive unit.
PATTERN ATLAS
Clinical Pattern Reading
Cross Compensation Loop
Restriction and protection transferred across the shoulder, thorax, abdomen, pelvis, and lumbar region.
Associated PatternScapular Lock
Chronic right shoulder compensation influenced thoracic rotation and trunk organization.
Secondary PatternAnterior Chain Lock
Anterior collapse and abdominal holding limited vertical extension and increased lumbar protection.
Base PatternPelvic Lock
Pelvic adaptation became part of the load-transfer problem expressed through the low back.
ENTRY STRATEGY
Treatment addressed the system, not only the painful area.
Shoulder Region
To reduce upper-body compensation and improve scapular-thoracic organization.
Abdominal Region
To reduce anterior chain holding and allow the trunk to regain vertical extension.
Lumbosacral Region
To release local guarding and support pelvic-lumbar reorganization.
Clinical Logic
The treatment focused on reducing the need for compensation, rather than forcing movement through the painful area.
CLINICAL TURNING POINT
After treatment, the body no longer needed to protect itself in the same way.
Immediately after the session, the patient reported a clear reduction in pain. The visible change was not limited to the lumbar area. The whole posture reorganized.
Protection decreased.
- Pain reduced
- Standing became easier
- Shoulder balance improved
- Abdominal holding softened
- Walking became less guarded
WHAT BECAME VISIBLE
Posture changed because the protection pattern changed.
Standing
Standing became more upright and less guarded.
Shoulder Balance
Right shoulder depression and asymmetry decreased.
Anterior Chain
Anterior trunk collapse and abdominal holding softened.
Pelvic Support
Pelvic alignment appeared more balanced.
Movement
Walking looked less protected and more confident.
CLINICAL REFLECTION
Acute pain often appears where compensation finally fails.
This case illustrates a central principle in Fasciapuncture® clinical reasoning: pain location does not always reveal pattern origin.
The patient came for acute low back locking, but the body showed a relationship between chronic right shoulder compensation, thoracic restriction, abdominal holding, pelvic adaptation, and lumbar protection.
When treatment reduced the need for protection, the system reorganized rapidly. The change was visible through posture, movement, and pain reduction.
FOLLOW-UP
One week later, he was still working normally.
Approximately one week after treatment, the patient reported that both the acute low back pain and the chronic shoulder discomfort had remained significantly improved.
More importantly, he had already returned to the physical demands of daily work: lifting supplies, organizing shelves, standing at the checkout counter, and managing the store throughout the day.
For a person whose work continuously challenges the musculoskeletal system, this follow-up provided a meaningful indication that the change was holding.
What surprised him most was the speed of the change. Having previously received treatment in China, he expected that improvement would require a longer treatment course.
Instead, a single Fasciapuncture® session produced a result that remained stable one week later.
KEY LEARNING POINTS
What this case teaches
Pain Location Is Not Always Pattern Origin
The lumbar region was the complaint, but the compensation involved shoulder, thorax, abdomen, pelvis, and lumbar protection.
Compensation Can Travel Across the Body
A chronic shoulder pattern may contribute to trunk rotation, pelvic adaptation, and low back overload.
Posture Can Reveal the System
The before-and-after images show how visible organization changed when protection decreased.
Release Is Often Systemic
The clinical shift was not only pain reduction, but a broader postural reorganization.
CONNECTED CLINICAL MAP
Related Patterns and Conditions
RELATED CONDITIONS
Symptoms that may share similar compensation patterns
RELATED CASES
Other cases showing postural reorganization and system release
CONTINUE LEARNING

