CLINICAL RESPONSIBILITY ESSAY
When a Patient Cries
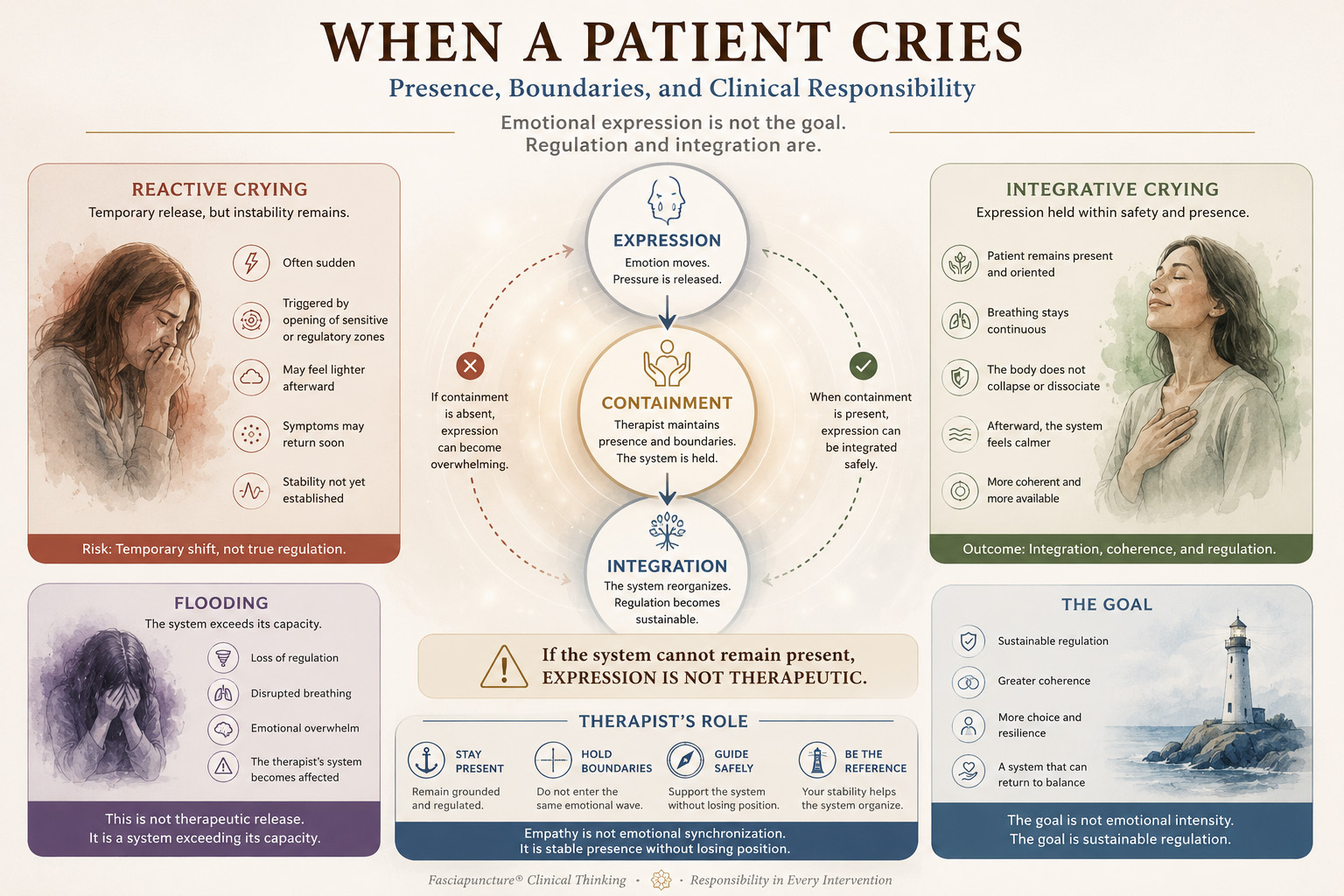
Presence, Boundaries, and Clinical Responsibility
Emotional expression may appear during treatment. But is crying always therapeutic? And what is the clinician's responsibility when a patient's system begins to open?
Expression is not always integration. Regulation remains the clinical goal.
THE CLINICAL QUESTION
Is Crying Always a Sign of Healing?
In recent years a common idea has become widespread:
The statement sounds compassionate. Sometimes it may even appear true.
Yet clinically, emotional expression alone is not a measure of regulation.
CLINICAL MOMENT
A Brief Clinical Encounter
A patient presented with lumbar pain, leg discomfort, visible anxiety, and systemic instability.
Following stimulation of a midline abdominal zone, the patient began crying intensely within minutes.
The reaction was immediate. The needle was removed. Manual contact replaced stimulation. Attention returned to containment rather than expression.
The session later resumed through more stabilizing fascial entry zones.
The patient left calm. The system remained coherent.
CLINICAL DIFFERENTIATION
Not All Crying Is the Same
Integrative Crying
The patient remains present. Breathing continues. The body does not collapse.
Afterward the system appears calmer, more coherent, and more available.
Reactive Crying
Often sudden. Frequently follows opening of regulatory zones.
Temporary relief may occur, but stability is not yet established.
Flooding
Loss of regulation. Disrupted breathing. Overwhelming emotional intensity.
The system is exceeding capacity.
The Risk of Crying Together
Some therapists believe that sharing the patient's emotional state demonstrates empathy.
Empathy is not emotional synchronization.
It is stable presence without losing position.
FASCIAPUNCTURE® OBSERVATION
Opening Is Not the Goal
Certain fascial zones, particularly along the anterior midline, may trigger powerful emotional responses.
The appearance of emotion does not automatically indicate integration.
Clinical observation suggests that some zones tend to open systems, while others tend to stabilize them.
The goal is not emotional intensity. The goal is sustainable regulation.
A Simple Clinical Principle
Emotional expression becomes meaningful only when it occurs inside a system capable of integrating it.
FINAL REFLECTION
Redefining Empathy
This is not distance.
It is responsibility.
And sometimes, the most compassionate act is simply remaining steady when someone else cannot.
RELATED CLINICAL PATTERNS
This reflection belongs to the wider Clinical Map
Global Protective State
When the body remains organized around protection and vigilance.
REGULATION PATTERNAutonomic Dysregulation
Where emotional intensity and physiological instability overlap.
CENTRAL PRESSURECore Block
Where breathing and emotional containment interact.
BREATHING PATTERNDiaphragm Restriction
A frequent contributor to emotional holding and protective tension.
CONTINUE EXPLORING
Regulation Requires More Than Expression
Explore how protection, autonomic regulation, breathing, and clinical responsibility interact within the wider Fasciapuncture® Clinical Map.
