SIGNATURE CLINICAL CASE
When the Foot Felt Electrified
A woman who could not tolerate socks, shoes, or even the touch of a blanket gradually recovered sensation, sleep, digestion, body weight, and confidence through systemic regulation over time.
CLINICAL OPENING
The pain was in the foot, but the source was not local.
A woman in her fifties arrived with an extraordinary complaint: her foot produced electric-shock sensations even with the lightest contact.
She could not wear socks. She could not tolerate a blanket touching her feet. The slightest friction triggered unbearable pain.
There was no swelling, no redness, no structural injury, and no visible local lesion. The presentation suggested hypersensitivity rather than a purely mechanical foot problem.
The foot was not the problem. It was the messenger.
INITIAL SYSTEM STATE
The Foot Was Expressing a System-Wide Sensory Alarm
Symptoms
- Electric-shock sensations in the foot
- Severe touch intolerance
- Unable to wear socks comfortably
- Unable to sleep with blankets touching the foot
Local Findings
- No swelling
- No redness
- No visible injury
- Marked hypersensitivity
Systemic Reading
- Distal sensory amplification
- Possible spine–foot fascial connection
- Neuro-fascial hypersensitivity
- Autonomic overactivation
Clinical Question
- Why was the foot so reactive?
- Was the painful area the origin?
- Could proximal regulation calm distal sensitivity?
PATTERN ATLAS
Patterns Revealed in This Case
Neuro-Fascial Irritation
The foot appeared hypersensitive because the sensory pathway was amplified.
02Posterior Compression
The spine–pelvis–leg chain may have contributed to distal sensory overload.
03Cervical Axis Tension
Cervical sympathetic tension may influence global sensory reactivity.
04Autonomic Dysregulation
The body remained in a protective state, amplifying touch and pain signals.
SPINE–FOOT CONNECTION ATLAS
The Foot Was the Site of Expression, Not the Site of Origin
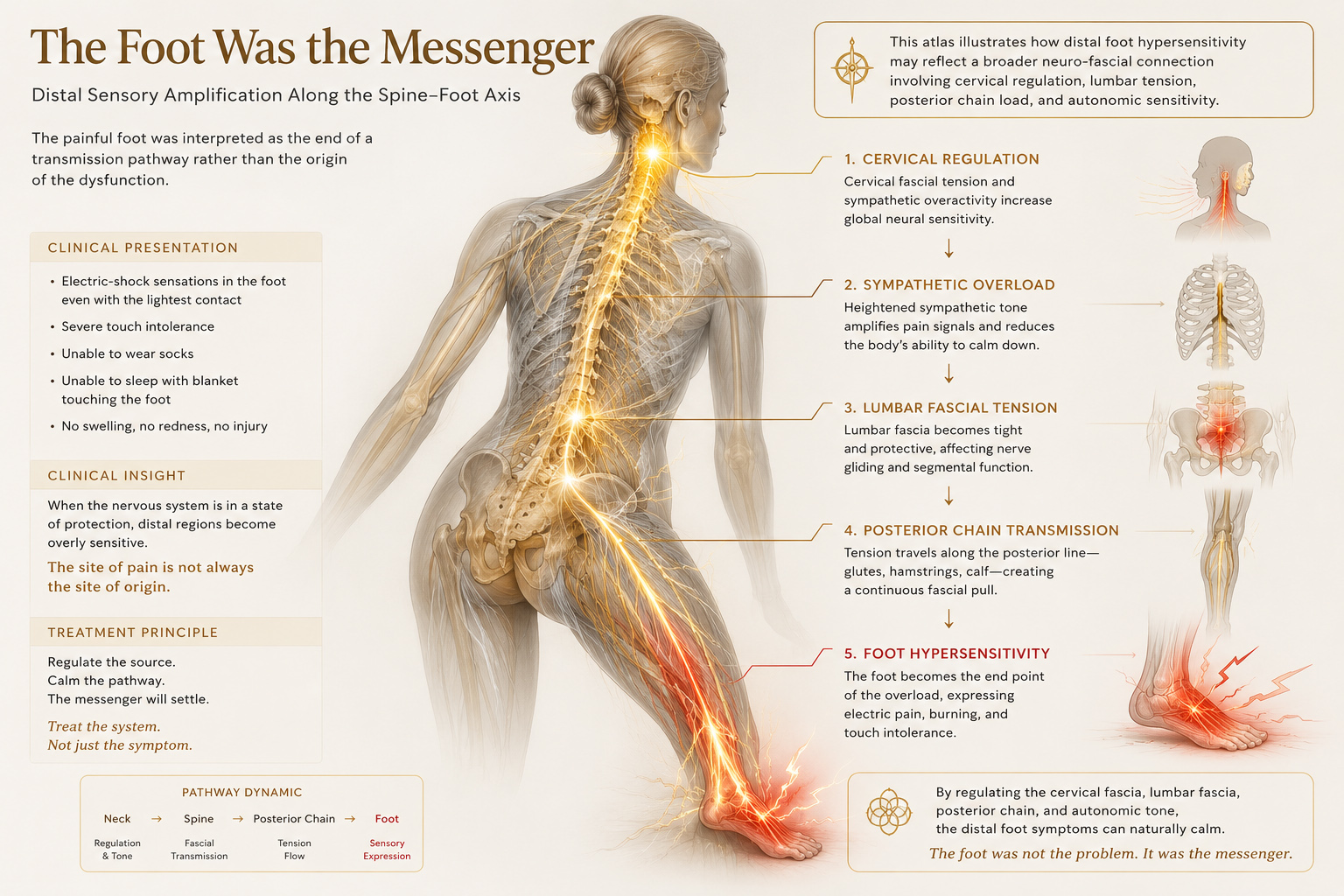
This case illustrates how distal foot hypersensitivity may reflect a broader neuro-fascial connection involving cervical regulation, lumbar tension, posterior chain load, and autonomic sensitivity.
CLINICAL READING
Why the source was not interpreted as the foot
The absence of swelling, redness, local trauma, or visible tissue injury suggested that the pain did not originate from a local inflammatory foot lesion.
Instead, the foot appeared to be expressing a state of sensory amplification. In such cases, the most painful region may be the end of a chain rather than the beginning.
Distal hypersensitivity often begins where the system can no longer regulate sensation.
ENTRY STRATEGY
Treatment Did Not Begin at the Foot
THE CLINICAL TURNING POINT
The First Change Was Not Strength
As the proximal fascial and autonomic tension softened, the foot gradually became less reactive. The patient could tolerate contact that had previously felt unbearable.
This suggested that the foot pain was linked to a broader sensory regulation problem, not merely a local foot disorder.
WHAT BECAME VISIBLE
The Foot Calmed When the System Calmed
LONG-TERM EVOLUTION
The Foot Was Only the Beginning
This case did not end with the reduction of foot pain.
Over more than ten treatment sessions, the patient's condition continued to evolve.
The electric sensations gradually became less frequent and less intense.
She began wearing socks again.
Later, she was able to wear shoes comfortably, even during the coldest winter months.
The hypersensitivity that once dominated daily life slowly disappeared.
CLINICAL REFLECTION
The Foot Was the Messenger
The painful foot was never interpreted as an isolated mechanical problem.
From the beginning, the symptoms were viewed within a broader context involving the nervous system, fascial tension patterns, autonomic regulation, and global adaptation.
Over time, improvement appeared not only in sensation, but also in sleep, digestion, body weight, and overall vitality.
This suggests that distal hypersensitivity may sometimes reflect a broader state of systemic dysregulation rather than a local foot disorder alone.
The foot was the messenger.
The recovery belonged to the entire system.
CONNECTED CLINICAL MAP
Explore Related Conditions & Patterns
RELATED CASES
Other Cases in the Same Clinical Map
CONTINUE LEARNING
From Foot Pain to System Reading
Foundations of Fasciapuncture®
Understanding why pain is not always the origin.
Module 2Clinical Assessment
Reading distal symptoms through global fascial patterns.
Module 10Lower Limb Disorders
Understanding foot, ankle, knee, and gait symptoms through fascial chains.
TrainingClinical Reasoning Pathway
Learn how cases become maps for clinical decision-making.