SIGNATURE CLINICAL CASE
When a Headache Is Not Only in the Head
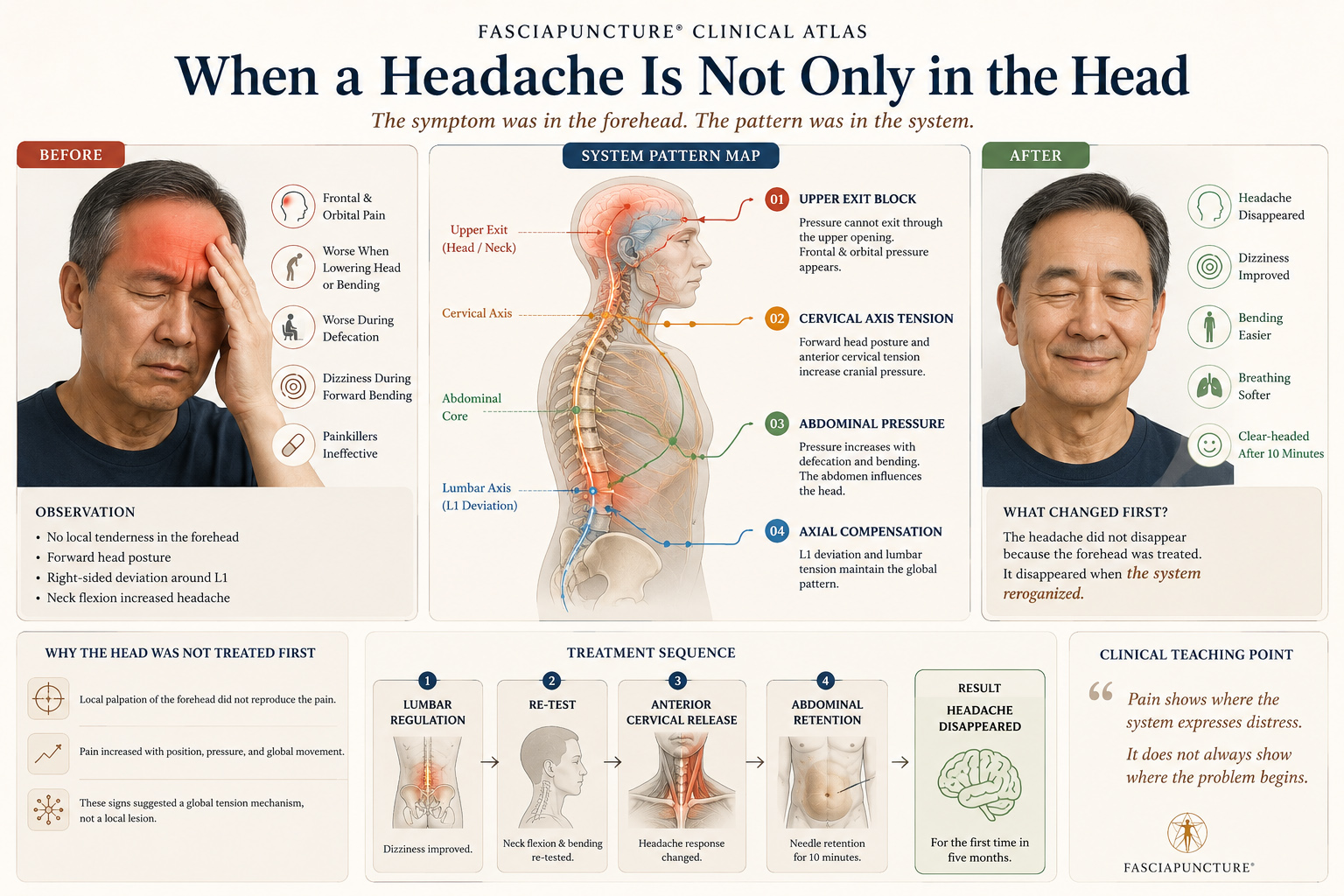
A 62-year-old man with persistent frontal and orbital headache for five months, normal examinations, no response to painkillers, and a clear shift after fascia-based clinical reasoning.
```
CLINICAL OPENING
The pain was in the forehead, but the key was not there
The patient, a 62-year-old man, had suffered from headache for five months. The pain was located mainly in the forehead and around the eyes. Despite multiple medical examinations, no clear explanation was found.
Painkillers were ineffective. Local palpation of the forehead did not reproduce the pain. This became an important clinical sign: the painful area was not necessarily the origin of the disorder.
INITIAL SYSTEM STATE
What the body showed before treatment
Main Symptoms
- Frontal and orbital headache
- Worsening over five months
- Painkillers ineffective
- No local tenderness on the forehead
Aggravating Factors
- Lowering the head
- Forward bending
- Defecation
- Dizziness during standing flexion
PATTERN ATLAS
The headache belonged to a pressure and axis pattern
Upper Exit Block
Frontal and orbital pressure, aggravated by lowering the head, suggested difficulty releasing pressure through the upper exit.
Cervical Axis Tension
Sitting neck flexion increased the headache, showing that cervical axis tension was involved in the symptom expression.
Abdominal Pressure
Defecation and pressure-related aggravation suggested that abdominal pressure was influencing cranial symptoms.
Axial Compensation
Forward head posture and right-sided deviation around L1 indicated that the head symptom was part of a larger axial adaptation.
BEFORE & AFTER CLINICAL ATLAS
When the system reorganized, the head became clear
Before
- Persistent frontal headache
- Orbital pain and pressure
- Dizziness on standing forward bending
- Forward head posture
- Right-sided deviation around L1
After
- Headache disappeared after rest
- Head felt clear for the first time in five months
- Dizziness improved after lumbar regulation
- Neck flexion response changed
- The system settled through abdominal retention
ENTRY STRATEGY
The treatment followed the functional signs
Lumbar Regulation
The L1 and lumbosacral region were addressed first because postural observation and bending response suggested an axial component.
Functional Re-Test
Neck flexion and forward bending were re-tested to observe whether the headache and dizziness changed after lumbar regulation.
Anterior Cervical Release
The anterior cervical fascial structures were treated after the cervical axis was confirmed as part of the symptom pathway.
Abdominal Retention
Abdominal needle retention for ten minutes allowed the system to settle, reduce pressure, and reorganize.
CLINICAL TURNING POINT
After ten minutes of rest, the headache disappeared
The dizziness improved after lumbar regulation. The headache then disappeared after anterior cervical and abdominal work.
After ten minutes of abdominal needle retention and rest, the patient reported that the headache had disappeared. For the first time in five months, he felt clear-headed.
WHAT BECAME VISIBLE
Observable signs of regulation
Head Pressure
The frontal and orbital headache disappeared after the system settled.
Dizziness
Standing forward bending became easier after lumbar regulation.
Cervical Axis
Neck flexion no longer behaved as a simple local neck problem.
Abdominal Pressure
The abdomen acted as a regulatory entry for cranial pressure.
System State
The patient felt clear-headed for the first time in five months.
CLINICAL REFLECTION
Pain shows where the system expresses distress
This case demonstrates one of the central principles of Fasciapuncture®: pain shows where the system expresses distress. It does not always show where the problem begins.
For persistent headaches with normal examinations, fascia-based clinical reasoning offers another way to read the body: through posture, pressure response, movement testing, and system regulation.
KEY LEARNING POINTS
What this case teaches
The painful area may not be the origin
No local tenderness in the forehead suggested that the symptom site was not the primary entry point.
Pressure response matters
Aggravation with bending, lowering the head, and defecation suggested a deeper pressure-regulation pattern.
Testing guides treatment
Neck flexion and standing forward bending showed how the headache connected to cervical and axial mechanics.
The abdomen may regulate the head
Abdominal retention allowed the system to settle and changed the cranial symptom without treating the forehead directly.
CONNECTED CLINICAL MAP
Patterns connected to this case
Upper Exit Block
Frontal pressure, orbital pain, head pressure, and upper cranial exit restriction.
Cervical Axis Tension
Neck flexion, forward head posture, and cervical-pressure relationships.
Abdominal Pressure
Defecation aggravation, pressure response, and cranial symptom expression.
Core Block
Central pressure, abdominal regulation, and systemic reorganization.
RELATED CONDITIONS
Conditions connected to this case
RELATED CASES
Other cases where the system became visible
When Breathing Becomes Quiet
A clinical moment where breathing descends and the system softens.
When the Abdomen Finally Let Go
A case of abdominal holding, breathing restriction, and pelvic protection.
After Wrist Surgery, the Problem Was No Longer the Wrist
Chronic arm pain, breathing restriction, and global anterior collapse after surgery.
CONTINUE LEARNING
From head pain to system reading
Module 1 — Foundations of Fasciapuncture®
Learn how symptoms become readable through fascia-oriented clinical reasoning.
Module 2 — Clinical Perception & Diagnosis
Learn to read posture, movement, pressure, and functional testing.
Pattern Atlas — Upper Exit Block
Explore how head pressure, neck tension, and cranial symptoms become connected.